

Abstract
Introduction: Even though the diagnosis criteria of chronic myelomonocytic leukemia (CMML) have been recently revised by the World Health Organization (WHO), recognition of this disease may be challenging. This myelodysplastic/myeloproliferative neoplasm can also be diagnosed by a relative accumulation of classical monocytes (cMO, CD14++CD16-) ≥94% of total peripheral blood monocytes and a decrease of intermediate (iMO, CD14++CD16+) and non-classical monocytes (ncMO, CD14lowCD16+) percentages measured by flow cytometry (Selimoglu-Buet, 2015; Talati, 2017; Patnaik, 2017; Hudson, 2018). However, inflammatory diseases concomitant to CMML or inflammatory state in CMML patients can provoke an increase of the iMO percentage leading to a decrease of the relative cMO percentage below the 94% threshold (Selimoglu-Buet, 2017). In these cases, the decrease of the relative ncMO percentage persists, hence it might be a useful diagnostic criterion relevant for CMML diagnostic. Since accurate delineation of the iMO and ncMO populations remains debated, the use of a ncMO specific marker, such as slan (6-sulfo LacNac), could be of interest.
Objective:We aimed to assess the clinical utility of the slan marker in peripheral monocytosis exploration and CMML diagnosis, especially in inflammatory state.
Methods: From November 2017 to July 2018, whole blood samples collected on EDTA or peripheral blood mononuclear cells (PBMC) were stained with the following antibodies as previously described: anti-CD45, CD2, CD56, CD24, CD14, CD16 (purchased either from Beckman-Coulter or Becton-Dickinson) and anti-slan (Miltenyi Biotec). Sample analysis was performed either with a Navios (BC) or a Fortessa (BD) cytometer. Fifty-four controls (19 young healthy blood donors and 35 age-matched healthy donors), 13 patients with reactive monocytosis and 37 patients newly diagnosed with a CMML were enrolled in this study.
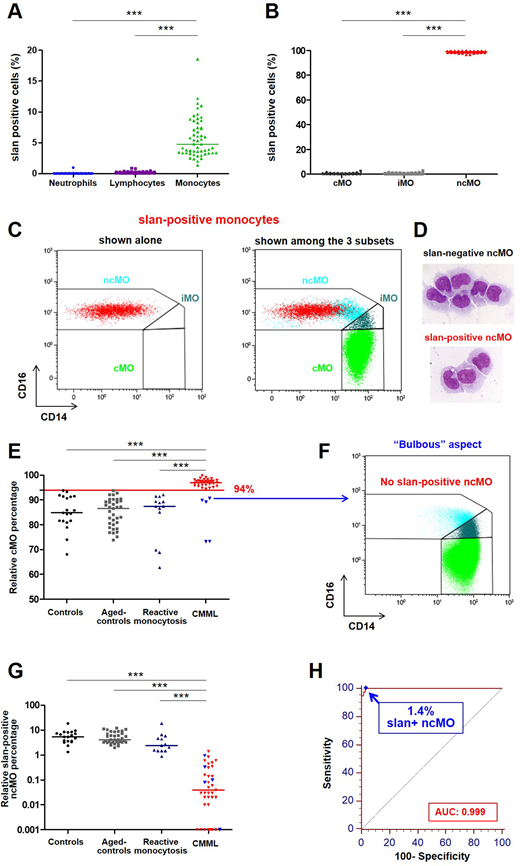
Results: Firstly, we analyzed the expression of the slan marker in the different circulating mature populations from control whole blood samples. We found that slan is only expressed in monocytes and not in neutrophils or lymphocytes (Figure 1A), especially not in NK cells. Among the three monocyte subpopulations, the expression of slan is restricted to ncMO with 98.9%±0.7% of slan-positive cells gathering within this subpopulation (Figure 1B). However, only 49.1%±12.3% of the ncMO are slan positive, corresponding to ncMo cells with the weakest expression of CD14 (Figure 1C, compare red population to blue one). Yet, both slan-positive and slan-negative ncMO subpopulations displayed similar morphological features after cell-sorting and MGG staining (Figure 1D).
Next, we assessed slan expression within the ncMO subpopulation in comparison with relative cMO percentage in healthy donors, patients presenting a reactive monocytosis or a CMML. Thirty-two out of the 37 CMML patients displayed cMO percentage above 94% as expected (Figure 1E). A significant decrease of slan-positive ncMO percentage was observed in CMML patients compared to healthy donors and patients with reactive monocytosis (Figure 1G). All the five patients whose cMO percentage was below the threshold (Figure 1E, blue triangles amongst red ones) displayed the well-recognized "bulbous" aspect (Figure 1F), with an increase of the iMO leading to the decrease of the relative cMO percentage. Interestingly, these patients that couldn't be diagnosed as CMML using the relative accumulation of cMO displayed a low percentage of slan-positive ncMO (Figure 1G, blue triangles amongst red ones).
Eventually, we established a Receiver Operator Curve (ROC) and obtained a 1.4% cut-off value of slan-positive ncMo with an area under the ROC curve (AUC) of 0.999 (Figure 1H). The use of the relative slan-positive ncMo percentage led to an improvement of the sensitivity of the CMML flow cytometry assay compared to the relative cMO% (100% vs 86%), as all the false negatives were retrieved.
Conclusion: Here, we describe a new parameter for CMML diagnosis, namely the decrease of the relative slan-positive ncMo percentage below 1.4%. This criterion, associated to the relative cMO quantification, may be useful, especially when CMML patient displays an inflammatory state.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal